“For physicians treating patients with atrial fibrillation who have undergone percutaneous coronary intervention with stent placement, it is paramount to balance the efficacy required with the risk of bleeding,” said Christopher Cannon, MD, cardiologist at Brigham and Women’s Hospital, lead investigator of RE-DUAL PCI™, and executive director of the Cardiometabolic Trials at the Baim Institute for Clinical Research. “Previously we did not have a lot of dedicated data on non-vitamin K oral anticoagulants in this setting; the results from RE-DUAL PCI™ are relevant to fellow physicians who care for these types of patients and are looking for an effective antithrombotic treatment regimen.”
The results were:1,2
-
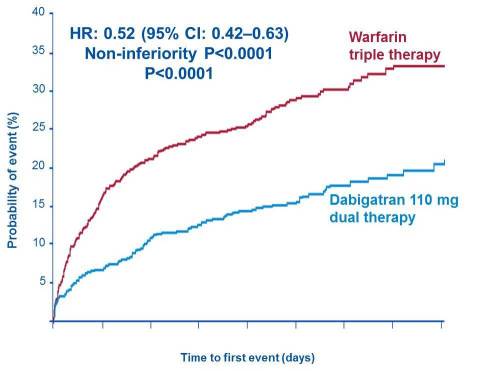
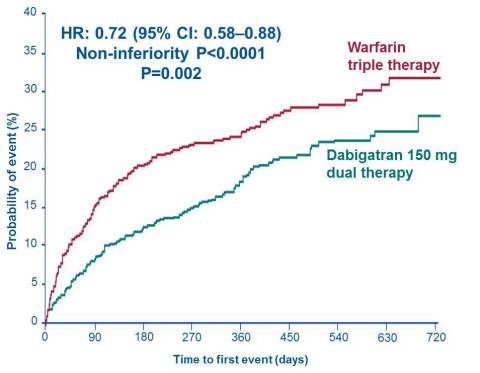
Incidence of primary endpoint (time to major or clinically relevant non-major bleeding event):
- 15.4% for Pradaxa® 110 mg dual therapy versus 26.9% for warfarin triple-therapy, which translates into a 48% lower risk
- 20.2% for Pradaxa® 150 mg dual-therapy versus 25.7% for warfarin triple therapy, which translates into a 28% lower risk
- Both Pradaxa® dual therapy groups also showed lower rates of major bleeding (when analysed alone, both for the ISTH* and the TIMI** major bleeding definitions) and total bleeding
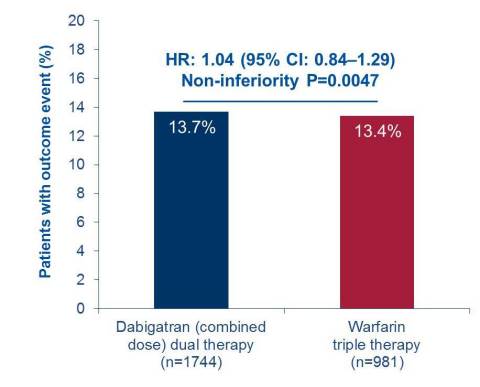
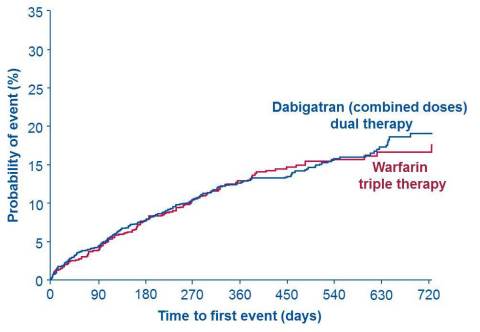
- Key secondary endpoint (combining death, myocardial infarction, stroke, systemic embolism and unplanned revascularisation):
- Similar rates of events were observed: 13.7% for the two Pradaxa® dual therapy groups combined, versus 13.4% for warfarin triple therapy
“The results we have seen from RE-DUAL PCI™ are another great piece of evidence on the benefit Pradaxa® can offer patients with atrial fibrillation and their treating physicians; a benefit which has been shown in many situations along the treatment journey,” commented Professor Jörg Kreuzer, Vice President Medicine, Therapeutic Area Cardiovascular, Boehringer Ingelheim. “Especially if you also take into account other recent data like the RE-CIRCUIT™ study in catheter ablation, evidence from ‘real-world studies’ or the results of the RE-VERSE AD™ study in emergency situations. Together, these data paint a really compelling picture of the safety and efficacy profile of Pradaxa.”1,2, 8-18
*ISTH, International Society on Thrombosis and Haemostasis
**TIMI, Thrombolysis In Myocardial Infarction
~ Ends ~
Please click on the link for ‘Notes to Editors’ and ‘References’: https://www.boehringer-ingelheim.com/RE-DUAL-PCI-ESC-2017
For more information, please visit: www.boehringer-ingelheim.com
Further Media Channels
www.facebook.com/boehringeringelheim